Autochthonous Chikungunya Fever in Traveler Returning to Japan from Cuba
To the Editor: Chikungunya fever is a febrile illness caused by
mosquito-transmitted chikungunya virus CHIKV: (genus Alphavirus, family
Togaviridae). Clinical signs and symptoms typically begin with
high-grade fever after an incubation period of 2–4 days (1). Other
common symptoms include polyarthralgia, which is usually symmetric and
involves multiple and distal joints, and skin involvement manifesting as
a macular or maculopapular rash (2). Peripheral lymphadenopathy (most
often cervical) and conjunctivitis might also occur (3).
Since late 2013, several outbreaks of illness caused by CHIKV have
occurred in the Americas, including South America, the Caribbean, and
the United States, which are outside this virus's former distribution
area (3). Although autochthonous transmission of chikungunya fever has
been reported in most Caribbean islands, only imported cases have been
previously reported in Cuba (4). As increased numbers of US tourists
visit Cuba after improved diplomatic relations in July 2015, reports of
chikungunya fever cases in Cuba are of interest for travelers and
healthcare providers. We describe a case of autochthonous chikungunya
fever in a man who had traveled from Japan to Cuba.
In late February 2016, a previously healthy 27-year-old man visited a
travel clinic in the National Center for Global Health and Medicine
(Tokyo, Japan) with fever and rash. In mid-February, he had traveled to
Havana and Santiago de Cuba in Cuba by way of Toronto, Ontario, Canada,
for 11 days of sightseeing. He used no insect repellent during the trip
and was unaware of any mosquito bites. When he sought care, he reported
a high-grade fever (39°C) for 24 hours and several symptoms since the
day of his return: retro-orbital pain, malaise, congested conjunctivas,
and a rash on his anterior chest. Over the previous few days, his knee
and ankle joints also had mild arthralgia.
Figure. Phylogenetic analysis of the chikungunya virus sequence obtained
from a patient returning to Japan (in bold) from Cuba in February 2016,
compared with reference sequences. Virus lineages are shown at right....
On physical examination, the patient's body temperature was 38.7°C, and
he had congested bulbar conjunctivas, cervical lymphadenopathy, and
maculopapular rashes on his face, trunk, and extremities (Technical
Appendix[PDF - 130 KB - 2 pages], Figure, panels A, B). Laboratory tests
revealed lymphopenia (701 cells/μL) and mild elevation of C-reactive
protein (0.87 mg/dL). Real-time reverse transcription PCR detected CHIKV
RNA in his serum sample. Phylogenetic analysis was performed on the
basis of nucleotide sequences of the E1 gene from the sample by using
the maximum likelihood method with 1,000 bootstrap replicates and MEGA
6.0 software (5). This sequence (GenBank accession no. LC146714) was
99.9% (1,319 of 1,320 sequences) was identical to that of a CHIKV strain
isolated from the Dominican Republic in 2014 (GenBank accession no.
KR559498) (Figure; Technical Appendix[PDF - 130 KB - 2 pages] Table).
The positive-to-negative ratio of CHIKV-specific IgM was negative in a
serum sample collected on day 4 after fever onset but was positive in a
sample taken 7 days later (positive-to-negative ratios 5.6 and 21.9,
respectively; ratios were considered positive if >11). Because the
patient's serum samples contained no dengue or Zika virus, infections
from these viruses were excluded, and chikungunya fever was diagnosed.
One day after the patient's first visit to the clinic, rashes on his
extremities became worse and slightly itchy. Pain also developed in his
wrists and metacarpophalangeal joints of his hand, followed by cervical
pain and slight rigidity on the hand's distal and proximal
interphalangeal joints. The patient was initially treated with
acetaminophen (600 mg 3×/d 2 d); after diagnosis of chikungunya fever,
he was treated with loxoprofen and rebamipide (60 mg and 100 mg,
respectively, 3×/d 7 d). The congested bulbar conjunctivas and rash on
his trunk improved; soon thereafter, all symptoms resolved.
CHIKV was first isolated in 1953 in Tanzania during an epidemic outbreak
in East Africa (6). Mosquitoes, predominantly Aedes aegypti and Ae.
albopictus, transmit the virus (2). Aedes spp. are also the common
vector of dengue and Zika viruses, and localized dengue outbreaks
occurred in Santiago de Cuba in 1997 and in Havana in 2000–2001 because
of the persistence of Aedes mosquito infestation in Cuba (7,8).
Furthermore, autochthonous Zika virus infection in Cuba was first
reported in March 2016 (9).
Differentiation between chikungunya fever, dengue fever, and Zika virus
infection is difficult because of similar signs and symptoms and common
endemic areas. We suspected chikungunya fever in this patient because of
high-grade fever and maculopapular rash, although he also had prominent
conjunctivitis, which is uncommon in CHIKV-infected patients but
frequent in persons infected with Zika virus (3,10). Phylogenetic
analysis of the virus isolated from this patient revealed a high
sequence homology with recent strains discovered in Caribbean and
Central American countries in 2014. Homology between the isolate from
this patient and a 2014 Asian lineage isolate from the Dominican
Republic was 99.92% at the nucleotide level.
This case highlights the potential threat of a chikungunya fever
outbreak in Cuba. Physicians should consider chikungunya fever in the
differential diagnosis for febrile travelers returning from Cuba with a
rash, similarly to patients returning from other countries in which
dengue fever, chikungunya fever, and Zika virus infection are endemic.
Preventive measures, including advice to travelers on proper use of
insect repellents, are critical for preventing CHIKV infection.
Motoyuki Tsuboi, Satoshi Kutsuna , Yasuyuki Kato, Eri Nakayama, Ken-ichi
Shibasaki, Shigeru Tajima, Tomohiko Takasaki, Yuichi Katanami, Kei
Yamamoto, Nozomi Takeshita, Kayoko Hayakawa, Shuzo Kanagawa, and Norio
Ohmagari
Author affiliations: National Center for Global Health and Medicine,
Tokyo, Japan (M. Tsuboi, S. Kutsuna, Y. Kato, Y. Katanami, K. Yamamoto,
N. Takeshita, K. Hayakawa, S. Kanagawa, N. Ohmagari); National Institute
of Infectious Diseases, Tokyo (E. Nakayama, K.-i. Shibasaki, S. Tajima,
T. Takasaki)
Acknowledgments
The authors thank the clinical staff at the Disease Control and
Prevention Center, Tokyo, Japan, for their help in completing this study.
A grant from the National Center for Global Health and Medicine
(27-6001) supported this work.
References
Burt FJ, Rolph MS, Rulli NE, Mahalingam S, Heise MT. Chikungunya: a
re-emerging virus. Lancet. 2012;379:662–71. DOIPubMed
Taubitz W, Cramer JP, Kapaun A, Pfeffer M, Drosten C, Dobler G,
Chikungunya fever in travelers: clinical presentation and course. Clin
Infect Dis. 2007;45:e1–4. DOIPubMed
Weaver SC, Lecuit M. Chikungunya virus and the global spread of a
mosquito-borne disease. N Engl J Med. 2015;372:1231–9. DOIPubMed
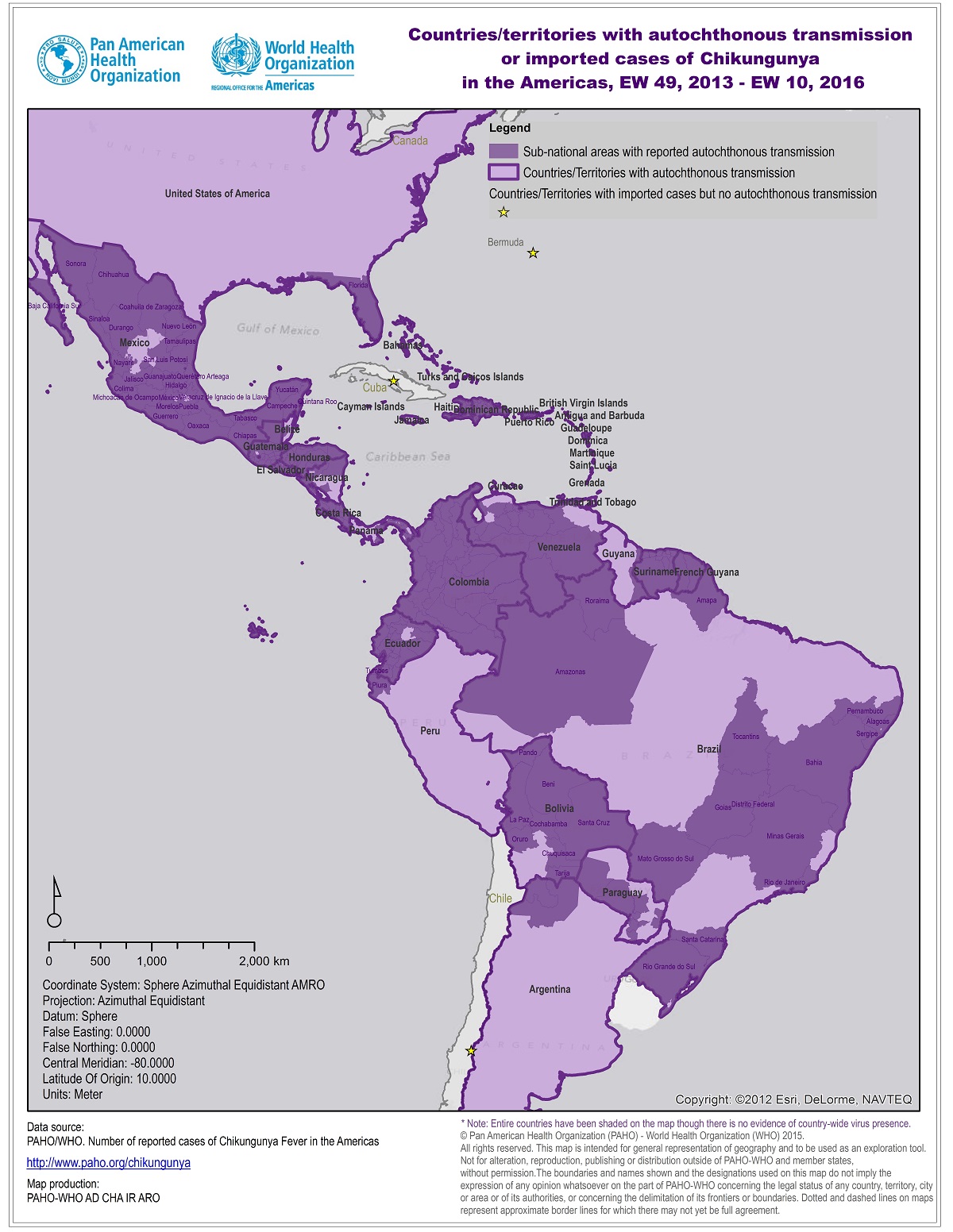
Pan American Health Organization. Countries/territories with
autochthonous transmission or imported cases of Chikungunya in the
Americas, EW 49, 2013–EW 10, 2016 [cited 2016 Apr 7].
http://www.paho.org/hq/images/stories/AD/HSD/IR/Viral_Diseases/Chikungunya/CHIKV-Data-Caribbean-2016-EW-10.jpg
Tamura K, Stecher G, Peterson D, Filipski A, Kumar S. MEGA6: molecular
evolutionary genetics analysis version 6.0. Mol Biol Evol.
2013;30:2725–9. DOIPubMed
Ross RW. The Newala epidemic. III. The virus: isolation, pathogenic
properties and relationship to the epidemic. J Hyg (Lond).
1956;54:177–91. DOIPubMed
Valdés L, Guzmán MG, Kourí G, Delgado J, Carbonell I, Cabrera MV,
Epidemiology of dengue and hemorrhagic dengue in Santiago, Cuba 1997 [in
Spanish]. Rev Panam Salud Publica. 1999;6:16–25. DOIPubMed
Peláez O, Guzmán MG, Kourí G, Pérez R, San Martín JL, Vázquez S, Dengue
3 epidemic, Havana, 2001. Emerg Infect Dis. 2004;10:719–22. DOIPubMed
Pan American Health Organization. Zika virus (ZIKV)—incidence and
trends. Regional Zika epidemiological update (Americas). 2016 Apr 8
[cited 2016 Apr 9].
http://www.paho.org/hq/index.php?option=com_content&view=article&id=11599&Itemid=41691&lang=en
Duffy MR, Chen TH, Hancock WT, Powers AM, Kool JL, Lanciotti RS, Zika
virus outbreak on Yap Island, Federated States of Micronesia. N Engl J
Med. 2009;360:2536–43. DOIPubMed
Source: Autochthonous Chikungunya Fever in Traveler Returning to Japan
from Cuba - Volume 22, Number 9—September 2016 - Emerging Infectious
Disease journal - CDC -
http://wwwnc.cdc.gov/eid/article/22/9/16-0603_article
{kind=link}
No comments:
Post a Comment